Listen to an audio version of this article:
By Margo Schulter
The presentation of a poster session advocating Intersex Genital Mutilation (IGM) at the recent Amsterdam meeting of the World Professional Association for Transgender Health (WPATH) has heightened a crisis of confidence and trust between the intersex and trans communities, with a special impact on those of us belonging to one or both communities who seek an equitable and productive alliance against the patriarchal tyranny of the sex binary.
My main purpose here as an endosex (nonintersex) transsexual woman is to explain for other endosex trans and/or nonbinary readers why we need to own our endosex privilege and understand the unique nature of intersex oppression, through IGM and other forms of childhood medical oppression, which we do not ourselves face, despite other aspects of our oppression which can and should make us “natural allies” of the intersex community. Indeed, intersex activists who are also trans like Cary Gabriel Costello, or who identify as nonbinary like Hida Viloria, embody this intersex-trans alliance, as does Organization Intersex International (OII), whose human rights commitments speak for the distinctive needs of the intersex community while also supporting the concerns of trans people, women, LGBTIQA people, and feminists at large.
After briefly focusing on the outrageous WPATH poster session and the larger context of the international struggle against IGM, I will address endosex privilege through some examples especially relevant to the trans community. This understanding of intersex oppression provides the needed context for appreciating the common ground that intersex people and many trans people share: the experience of inhabiting bodies that often violate social expectations of binary body sex. To help rebuild and strengthen an effective intersex-trans alliance, I will then outline some urgently needed WPATH reforms which members of both communities could support together — but which, I stress, must especially grow out of direct dialogue between members of the intersex community and WPATH.
An outrageous poster session: IGM as a human rights violation
IGM, a close relative in the world of human rights violations and sexism to Female Genital Mutilation or FGM, is non-consensual and indeed coercive surgery performed on intersex infants or children, not to address rare situations of urgent medical necessity, but to bring congenitally sex variant bodies in line with the patriarchal ideology of the sex binary. Like victims of FGM, victims of IGM suffer from the pain and trauma of genital cutting, from frequently reduced or lost sexual sensation, and from their bodies always showing the marks of a social system that devalues people with sexed characteristics like theirs. The physical violence and enduring psychological trauma inflicted by IGM have been described by its survivors, who are the ultimate authorities, as in this foundational document closely tied to a landmark event in intersex activism and visibility which I will detail shortly:
Intersex people, those deemed to have been born with bodies outside the categories of “standard” female or male, make up a portion of the population estimated at least somewhere around 0.7% by conservative criteria (Cary Gabriel Costello), or 1.7% (Anne Fausto-Sterling), with 1% or so being a helpful rounded figure. Writing for The Intersex Campaign for Equality, the affiliate in the United States of the Organization Intersex International (OII), Hida Viloria thus concludes that being intersex is “about as common as having red hair” in a country such as the USA.
While intersex is always congenital, not all intersex variations are identified at birth or during childhood, nor do all involve “ambiguous genitals.” Viloria cites an estimate that IGM may occur to one or two of each thousand persons born, a rate of 0.1-0.2% — a violent and coercive human rights violation of the most intimate kind which no one should endure! Both the United Nations and the European Union have affirmed the arguments of intersex advocates by declaring IGM to be a human rights violation.
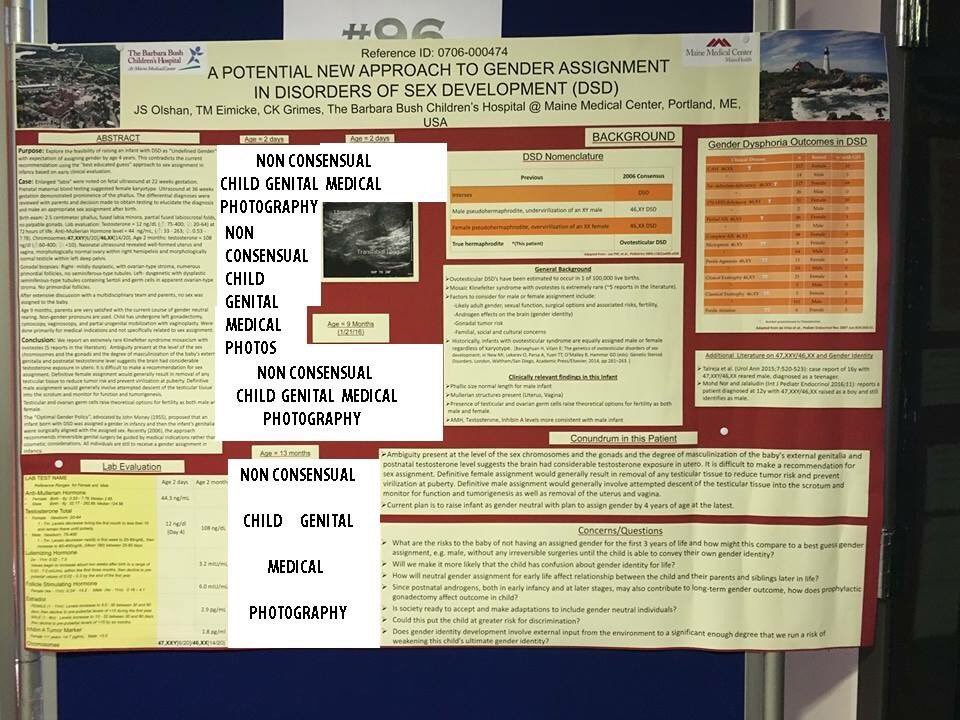
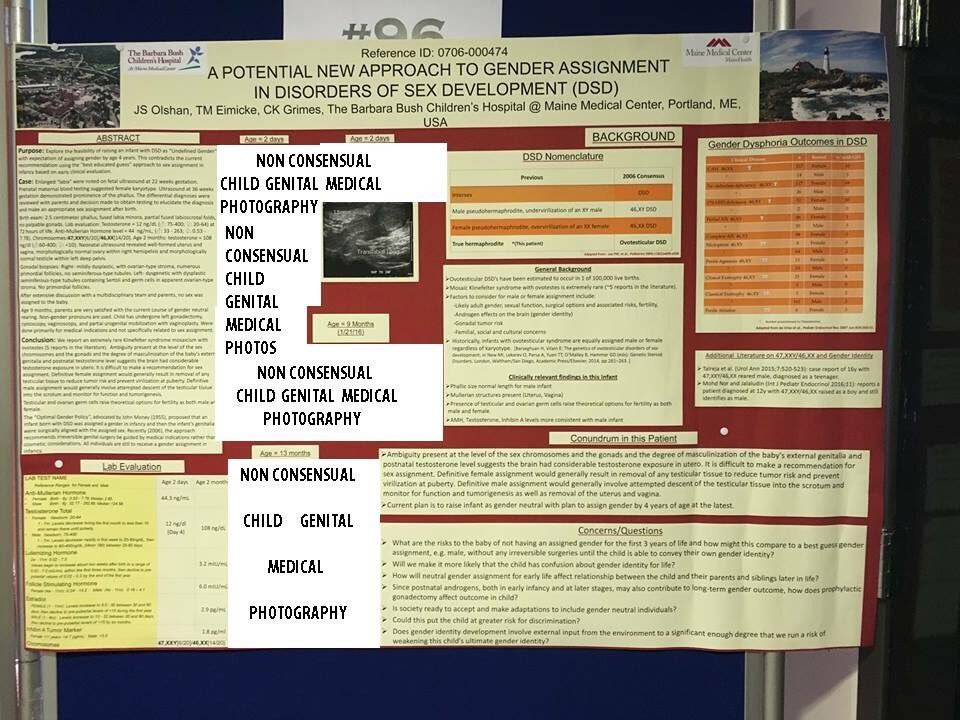
Adding insult to injury, the poster session at WPATH not only sought to justify this practice, at once barbaric and distinctly modern in its dependence on medical technology and expertise only developed around the mid-20th century but featured the graphic violation of its young victims’ privacy. The offending poster included close-up photographs of the genitals of intersex children, sometimes being grasped by medical professionals. Intersex activists documenting this sad display rightly edited out these violations of privacy and human dignity, replacing images with notices of “Non Consensual Child Genital Medical Photos.”
As if to make this display of professional ignorance and arrogance yet more sad, it occurred only a few months before the 20th anniversary of a watershed event of intersex activism and courageous visibility: the demonstration by intersex people and allies against IGM in October 1996 at the Boston meeting of the American Academy of Pediatricians. At that time, the Intersex Society of North America (ISNA) was in the forefront of intersex activism, a role now played, for example, by OII. Among allies present were members of the Transexual Menace.
The poster session at WPATH, 20 years after the Boston action, engaged in speculation about risks of “confusion about gender identity for life” that could result from a “neutral gender assignment” — rhetoric that reminds me as a Lesbian feminist of concerns raised not so long ago about marriage equality, called “genderless marriage.” Even more to the point for those of us in the trans community, the assumption that genital configuration determines gender identity is fundamentally opposed to our entire life experience. In fact, organizations like ISNA and OII have not opposed tentative binary sex designations for intersex infants, provided that the children are free to declare their own identities and to make their own informed decisions at an appropriate age about any surgeries they may (or may not!) choose. However, the poster session provided a forceful reminder that “sex assignment” has been and remains a frequently used euphemism for IGM, something that no medical professional should have the power to do or authorize without the fully informed consent of the person whose body is on the line.
An element of the poster session unfortunately connected to the current practice of WPATH itself is the use of the term “Disorders of Sex Development” (DSD), a term offensive to the intersex community and its allies as pathologizing natural intersex variations, just as the now-obsolete “Gender Identity Disorder” (GID) pathologized human variations in sex or gender identity. In 2006, some intersex people and allies reached a compromise with a group of medical professionals in favor of the DSD concept — a compromise which it was hoped by some of its supporters would help to end the practice of IGM, but was highly controversial at that time, and has since proved unhappy and inauspicious at best. Some intersex people have made an effort to live with the DSD acronym by interpreting it to mean “Differences of Sex Development” or “Diversity of Sex Development.” Most advocacy groups, however, use the term intersex. And all leading intersex organizations reject the “disorder” label, as WPATH must as well. Eliminating “disorder” language from the WPATH Standards of Care, and substituting language arrived at through a process of dialogue with the intersex community, is one step that will help to repair the damage done at Amsterdam.
One reason why IGM is wrong should be of special interest to WPATH: the way it engenders a special kind of sex or gender dysphoria that is iatrogenic, or itself caused by medical treatment. Here that “treatment” is the child abuse of IGM, which when done in infancy may well alter a child’s body in what proves to be the wrong direction when that child is old enough to know and express a sex identity. Further, any “direction” of medically enforced genital alteration typically proves to be wrong, because many intersex individuals, including individuals who are spared IGM and come to identify with whatever binary sex was designated at birth or in infancy, feel no need for any surgical alteration of their sex variant bodies. However, it must always be emphasized that IGM, like FGM, is objectionable for the pain, trauma, and social stigma it inflicts, and the personal autonomy it coercively violates, quite aside from issues of gender identity or sexual orientation, etc.
As a well-informed WPATH professional who supports intersex concerns put it to me, borrowing the language of many intersex people and allies, IGM is done to address not any dysphoria felt by an intersex infant or child, but the dysphoria and distress of professionals who cannot abide the reality of bodies outside the sex binary. It is the intersex person, however — and not these professionals, or even their parents often influenced by their prejudices and false expertise — who alone can and must weigh the risks of surgery, including lost or diminished sexual sensation which is always a possibility (as in surgery for endosex trans people also), and decide if the benefits outweigh these risks. Ironically, these risks of lost or diminished sensation are higher in infancy, because the structures are tiny, with nerves more likely to be severed. Thus the need for an infant to give informed consent is especially pressing — and, of course, impossible.
It is important for endosex trans people to understand that in today’s Western societies, which frame sex and gender as binaries, intersex people like endosex people most commonly view themselves through this lens, identifying as whatever sex was designated for them, with or without IGM. Although the percentage of intersex people who do not at maturity identify with their binary sex assigned at birth is somewhat higher than the percentage of endosex people who at maturity identify as trans, and some in either group identify as nonbinary, the majority of people in both groups alike do accept their binary sex designated at birth. Indeed, when adult intersex people face decisions about possible surgery, the issue is often not that of transition but whether to bring their bodies closer to “standard” expectations for the sex in which they have lived their entire lives. For example, an intersex woman might face the question of whether to have a vaginoplasty, a procedure no longer routinely performed as a form of IGM on intersex children before puberty because of “poor outcomes”; and, more rarely, of whether to have a clitoral reduction, given the tragic prevalence of this form of IGM.
Viewing intersex primarily as a question of “gender identity” obscures both the critical importance of outlawing IGM and other forms of childhood medical abuse and the nature of many of the medical decisions faced by intersex adults. It is possible to recognize the real overlap between the membership and concerns of the intersex and trans communities without losing sight of this larger perspective. The following guidelines from the Intersex Campaign for Equality (OII-USA) are helpful on these and other points:
It is also sobering to reflect that despite 20 years and more of dedicated intersex activism, only two countries have so far outlawed IGM: Malta and Chile. WPATH has the responsibility to speak out against IGM, a responsibility shared with the trans community at large. Active allyship is the best and indeed the only way to rebuild an effective alliance after the debacle at Amsterdam.
Owning endosex privilege: Two examples
As a transsexual woman and Lesbian feminist with white and endosex privileges, I face a number of oppressions: but not racism, and not intersex oppression. To illustrate endosex privilege as it applies to endosex trans people, I have chosen two scenarios, the second of which is based on my own situation as compared to that of an intersex person.
The eager trans child: informed consent and “watchful waiting”
Much antitrans literature, some of it sadly produced in the name of feminism, features sensational stories about young children undergoing sex reassignment surgery. These surgeries are, indeed, an everyday reality, but for intersex infants and children rather than endosex children who may be trans or gender nonconforming (GNC).
Let us consider an endosex child at the age of 7 who expresses a very strong cross-sex identity, and has done so since the age of 3 or 4, when first old enough to articulate a sense of sex or gender. Katy was designated male at birth, but has always insisted not only that she wants to transition, but that she is a girl. She has very diverse interests, and isn’t much concerned with conventional gender roles, but makes it very clear that whatever she’s doing, she does as a girl.
Further, having had time to get to know and understand this situation, her parents enthusiastically support her sense of female identity, and also give positive reinforcement for her flexibility about gender roles and interests by sharing with her feminist classics like “Free To Be You And Me.”
Coming from this positive outlook, Katy and her parents have a proposal for the professionals at the supportive Gender Identity Center (GIC) they’ve found in their community. Why not arrange for her to have sex reassignment surgery as soon as possible, within the next year? This will resolve the body dysphoria that she experiences, as well as further solidifying her social identity, for example at her school where her identity as girl is widely respected by teachers and peers, although there hasn’t yet been a formal transition.
Doubtless, the GIC professionals would explain that while a formal social transition looks like a very constructive option, surgery at this point is both unnecessary and unethical. The simple reason is that Katy, no matter how strongly or confidently she identifies and lives as female, is not yet old enough to exercise the informed consent that surgery requires. Her parents, as loving and well-intentioned as they are, cannot make this decision on her behalf: only she can do that, when old enough to fully to appreciate the risks and consequences.
And “watchful waiting,” to use the words of the WPATH Standards of Care, also gives Katy the time and space to test and confirm her identity and intentions during the remainder of her childhood years, with social transition as an excellent “Real Life Experience” (RLE) to assist her in this process. Medical decisions can thus be keyed both to the necessities of her physical development and her maturing ability to consent in an informed way. At puberty, she will have the option of blockers to delay sex development in an undesired direction; then, at 16, she can begin cross-sex hormone therapy, with surgery an option beginning at age 18.
Although Katy and her family may find this delay in surgery a bit frustrating, we understand that it is meant to protect her autonomy and ability to make fully informed and mature decisions, given the irreversible nature of surgery as well as its nontrivial medical risks. A professional might also reassure the eager parents that trans kids are quite capable of getting through childhood and adolescence before having surgery without any risk of “lifelong gender confusion” — especially when parents, teachers, and friends are supportive, as is certainly the case here!
Contrast this ethical refusal to do genital surgery on a child, despite the enthusiastic desire of child and parents alike, with the routine readiness of professionals to perform IGM on intersex infants and children who typically are not yet old enough to know or express their identities and wishes, based on notions “by guess and by golly” of how the child’s identity might develop. What could be a clearer indication of the small valued placed on either the personal autonomy or bodily integrity of intersex people?
Again, I emphasize that the scenario of Katy at age 7 and her family seeking sex reassignment surgery is hypothetical and contrafactual. The whole point is that IGM needs to become equally so throughout the world. The fact that IGM is instead still widely practiced, and can be promoted at a WPATH meeting, is one cardinal measure of intersex oppression and endosex privilege.
If I had been born with my present anatomy
Another way of illustrating endosex privilege and intersex oppression is very personal to me. Weighing my options as a male-to-female transsexual for surgery, I decided on a procedure that would create a vulva including a sensate clitoris (on cliteracy, see CLITERACY, 100 Natural Laws), but without vaginal depth. For me, penetrative sex is not a priority –and I should emphasize as a Lesbian that many other transsexual Lesbian women do choose to have a full vaginoplasty. Given my own preferences and priorities, the simpler procedure had the advantages of being much less invasive, with an easier and faster recovery, as well as no issues of vaginal dilation to deal with.
Although I might well have reached the same decision without any knowledge of the intersex community, in fact becoming an intersex ally as I considered my medical options played a very important part in reinforcing my choice and the reasoning behind it. What especially moved me, as I recall, was the story of a woman with Androgen Insensitivity who had been assigned and raised female without IGM, identified and lived as a woman, and as an adult faced the question of whether or not to seek a vaginoplasty to make her body more heteronormative. After careful consideration, she decided that her body needed no modifications.
In the process, I also encountered a classic essay by Anne Fausto-Sterling, a writer on the topic of sex and gender and an ally of intersex people, where she noted that IGM is often based on a patriarchal preference for “penetration without pleasure” rather than “pleasure without penetration.” Those phrases stuck with me through the months of planning and making arrangements for surgery.
Now having been through that surgery, I have what I sought: the wonders of an independent female sexuality of a kind consistent with who I am, albeit neither reproductive nor confirming to standard sex binary or heteronormative expectations. And no one is seeking to intervene and alter my body without my consent — for example, to enforce a full vaginoplasty.
Now consider what might have happened had I been born with substantially similar genitals, as might have happened with some well-known intersex variations. In that case, a nonconsensual vaginoplasty “for my own good” and future participation in “normal sex” with men — and how dare you presume that I’m going to grow up and be heterosexual! — might well be my fate. In other words, I could be a prime candidate for IGM as usual.
The fact that no one is seeking to alter my body against my will is an inestimable endosex privilege. My concern –which should also be WPATH’s– is that intersex people also enjoy this elementary human right of bodily self-determination.
Common ground: Bodies with variant sex characteristics
While intersex oppression and especially the cardinal oppression of IGM and childhood medical abuse are unique, there is also a common ground shared by intersex people and many endosex trans people. More specifically, it is shared with those of us who are endosex trans and physically transition through hormones, and often also surgery: the experience of inhabiting bodies with intermediate sex characteristics.
Intersex people, by definition, have sex variant bodies at birth, while endosex trans people obtain sex variant bodies as a result of consensual medical interventions. Feelings of fear or aversion directed at such bodies, and those of us who inhabit them, are thus an important factor fueling IGM and other manifestations of interphobia or endosexism; and also transphobia in one of its aspects.
This aspect of transphobia comes to the fore when it is argued that hormones and surgery cannot really “change sex” because trans women and men who choose surgery (nonbinary trans people are more rarely brought into this argument) still retain some aspects of the sexed attributes present at birth, and thus do not measure up to our culture’s standards for a “real” (i.e. endosex) woman or man. The absence of reproductive organs and capabilities typical of a “real woman” or “real man” is a favorite theme.
To say that interphobia and transphobia share this common theme does not mean that they are identical. For example, some self-identified feminists who would be ready to accept as a woman an intersex person raised as female, especially if she is not too assertive about her intersex status and variant sex characteristics, would reject trans women because of our “male socialization.” And, as the WPATH poster session indicates, there are people, including medical professionals, who in some sense support trans rights while utterly disregarding those of intersex people.
Some binary trans people who seek surgery, as in my case, choose options other than those approximating as closely as possible the “standard” anatomy of the sex into which we have transitioned. For example, many trans men who choose to have genital surgery opt for a metoidioplasty. This procedure is based on the biological reality that almost all humans share in common the organ known as a phalloclitoris, to use a term familiar in the intersex community. The “standard female” form known as a clitoris and the “standard male” form known as a penis, as well as the many intersex variations along this continuum, are comparable in size and complexity. The difference is that a standard clitoris is mostly internal, with only a small portion external and thus visible, while a standard penis is more externalized. Dr. Helen O’Connell of Australia and her colleagues have, since the 1990s, documented the true size and complexity of the clitoris, with feminists such as Sophia Wallace and intersex educators such as Cary Gabriel Costello making her liberating findings more accessible.
In metoidioplasty, a trans man who has already been on testosterone therapy for some time, causing the external portion of the phalloclitoris to enlarge, receives surgery to release this external portion so that it takes on the qualities of a penis. An advantage of metoidioplasty, as opposed to a full phalloplasty aiming at a closer approximation of a “standard” male appearance, is that it is a simpler and less invasive procedure, focusing more on a comfortable embodiment for the individual than sex binary or heteronormative standards. This is in no way to question the preferences of many binary trans people who seek to approximate “standard” female or male anatomy and function as closely as possible, but only to recognize the range of preferences among trans women and trans men alike, not to mention nonbinary trans people who seek surgery.
Further, endosex trans people who seek hormone therapy but not surgery also arrive at sex variant states of embodiment which may call forth some of the same fears and prejudices as intersex variations — but without the threat of IGM, of course!
Members of the intersex community have presented a very useful concept, that of “sex characteristics,” which is also helpful for endosex trans people dealing with the reality of sex variant bodies. As Hida Viloria and Dana Zzyym explain , people may be born with standard female or standard male or intersex sex characteristics — and identify, if intersex, as female, male, or nonbinary. Endosex people show the same diversity. Likewise, those of us with voluntarily altered sex characteristics may identify in different ways: while I identify as a trans woman or trans female with mixed or variant sex characteristics, another endosex trans person with similar characteristics might identify as nonbinary, genderqueer, or gender fluid, etc.
Viloria and Zzyym are writing to affirm the right of intersex people to identify as they choose, and especially as nonbinary or specifically “intersex,” emphasizing that the abusive intervention of IGM is not only immoral but often fails to produce the “hetero-normative, gender-conforming outcomes” it’s advertised to promote. At the same time, in recognizing that many intersex people do not identify in this non-binary way, but rather “as men or women,” they embrace a larger alliance:
It makes perfect sense to those of us who know, love, and/or support trans people. We realize folks don’t always grow up to identify as the gender associated with the biological sex traits they were born with.
The common ground of sex variant embodiment can invite a natural alliance between the intersex and trans communities, provided that endosex trans people act as real allies, and are ready to understand and join in the struggle against IGM and related forms of childhood medical abuse that make intersex oppression unique. It is also our responsibility as endosex trans people to recognize the special prejudices and hurdles sometimes faced by those intersex people who do seek as adults to transition and to help them in the task of educating medical professionals that intersex and trans are overlapping or intersecting rather than mutually exclusive categories.
That the common ground of sex variant embodiment can lead to conflict rather than harmonious alliance, especially when endosex trans people fail to understand and act on the realities of intersex oppression, is not a new problem. This problem has a number of aspects or areas of concern, one of which I can speak to from personal experience.
Since physical sex is a spectrum, the endosex/intersex distinction is itself arbitrarily constructed, one reason why estimates on the percentage of intersex people are necessarily imprecise, being in good part a question of definition. Under patriarchy, where intersex is seen both as an undesirable condition and as a threat to the sex binary, the criteria tend to be rather narrow and conservative. However arbitrary and indeed illusory this attempt to make a binary out of a spectrum may be, however, the consequences of being deemed intersex under modern Western patriarchy are all too real and concrete, from IGM and the lifelong social stigma it reflects and enforces to extra difficulties in accessing necessary healthcare.
During my adolescence, I developed mild gynecomastia and found this pleasant as someone designated male at birth who had expressed a desire to transition at age 4. A teacher at school encouraged me to wear a top when swimming so that the boys wouldn’t make fun of my breasts, something I enjoyed as rather like a “third gender” status. Before starting hormone therapy in 1972 at age 21, I had the opportunity to join a study and be tested for intersex variations, a possibility raised by my gynecomastia and also a finding that I was sterile (aspermia) — a finding, however, that could arise from causes like childhood infectious diseases. Chromosomal and other tests revealed no intersex variations.
The best way to describe my situation might be to say that I am an “endosex variant.” My gynecomastia made my adolescence as a mostly closeted trans person (both internally and socially) a bit easier, and definitely helped when I transitioned in 1972-1973 and estrogen therapy proved very effective. What my sex variation did not do was to make me vulnerable to anything like intersex oppression. If I had been threatened as a teenager with coercive breast reduction surgery, there might be more of a comparison, but no such thing happened. And while my breast development before transitioning might have led to a bit more teasing and harassment in my high school years, gender identity and expression were clearly the main issue. One man who was a counselor told me at age 16 that I had obviously “been raised by women,” and was “on the feminine side,” a situation he hoped to help remedy. My minor sex variation was not the focus of concern.
Today I find that the term “endosex variation” nicely describes whatever biological condition led to my adolescent gynecomastia and then made my hormone therapy more effective in feminizing my secondary sex characteristics. Back in 1973, the line between this and intersex was not so clear to me, although in discussing my sex variation I made it clear that doctors had found no intersex condition. Looking back, I reflect on my utter cluelessness at the time about the nature of intersex oppression, especially IGM and childhood medical abuse in general! I shared this cluelessness with other endosex Second Wave feminists, and indeed with endosex people generally, a situation remedied only when intersex people themselves visibly confronted and challenged the violence of IGM, through events such as the 1996 demonstration in Boston.
Thus the first area of concern in intersex-trans relations is for endosex variant trans people like me to celebrate our sex variations while recognizing that they are very different in their consequences under modern Western patriarchy than intersex status and oppression. More generally, many trans people including myself, when approaching transition, may have a desire to seek and find any biological condition that might “explain” our cross-gender identity. This was true despite my strong feminist awareness that physical sex and gender are two quite different things, as trans people should especially know.
The second aspect concerns endosex trans people who unfortunately carry an interest in sex variations and the intersex community a step much too far, by claiming intersex variations they do not have. This kind of intersex misappropriation is compounded in its harm when those doing it claim intersex variations of a nonexistent kind, such as the ability to reproduce through self-fertilization, spreading misinformation where ignorance and misconceptions are already all too prevalent. Worse yet, the ignorance of medical providers can be so great that myths spread by intersex misappropriators can put at risk or even cost lives. A deadly example is the myth that Congenital Adrenal Hyperplasia does not have a salt-losing or salt-wasting form causing a life-threatening condition of hyponatremia or low sodium which must be medically treated and managed properly to save the person’s life!
A third aspect concerns the sometimes delicate line between the celebration of intersex and other bodies with variant sex characteristics, and the fetishization of intersex people. Like the fetishization of trans people, intersex fetishization should not be confused with a real appreciation for the unique beauty of intersex people and bodies — as opposed to the violence and abuse of IGM and intersex stigma, which like the abuse of trans people can sometimes go hand in hand with fetishization and sexual objectification.
What ties all of these aspects of intersex-trans understanding (or its absence) together is the reality that intersex under modern Western patriarchy is neither an identity, although some intersex do identify their gender as intersex; nor even simply the current physical condition of having variant sex characteristics deemed outside the binary (as I do after surgery). Rather, it is a congenital condition that leads to the risk and reality of stigmatization and medical abuse, including IGM, through the uniquely vulnerable developmental period of infancy, childhood, and adolescence. From this foundational realization, the intersex and trans communities can build a harmonious alliance.
One productive focus for this alliance is in addressing the problems that intersex people face in obtaining the medical care they seek and need. Such medical care can include routine health maintenance, and psychological care supporting people in dealing with social stigma, as well as transition for the relatively small but substantial minority who seek it.
Until recently, the traditional diagnosis of Gender Identity Disorder (GID) not only imposed social stigma on the trans community but raised a special obstacle for intersex people seeking to transition, because they were explicitly excluded from this diagnosis that was so often the key to accessing treatment. Indeed, intersex people found themselves forced to conceal their intersex status from gatekeepers in order to obtain “the letter” with a diagnosis of GID that was a passport to transition care services. Seeking transition care based on one’s intersex condition was not an option, because practitioners focusing on the treatment of “Disorders of Sex Development” (DSD) were and are heavily invested in the ideological belief that intersex people will invariably identify with their birth-assigned sex, the “assignment” generally involving IGM, regardless of what intersex people themselves may say in asserting their trans identification.
If there is to be true honor and mutual alliance among people with variant sex characteristics, then WPATH is a fitting arena for action. In attempting to outline some themes for this action, I emphasize early and often that only the intersex community can set the agenda and then actualize it through direct dialogue with WPATH, with endosex trans people playing a vital supporting role in this process.
Liberating WPATH: Some tentative ideas
One response I got in discussing the WPATH poster session promoting IGM is that closer vigilance should have been exercised about who is invited to present such sessions. While this is surely true, repairing the damage done will involve much more than avoiding such overtly interphobic presentations in the future. It will involve WPATH taking its proper leadership role in calling for the outlawing of IGM, ending the use of pathologizing terms such as “disorders of sex development,” and also fostering professional education and cultural competence in support of better and more responsive care for those intersex people who do choose to transition, whether in the wake of IGM or otherwise.
IGM and iatrogenic sex dysphoria: WPATH must take a stand
In Section XV of the current WPATH Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7 (2011), the portion addressing issues of gender dysphoria in intersex people, some differences in treatment between intersex and endosex people who wish to transition is noted. As the authors note:
One reason for these treatment differences is that genital surgery in individuals [who are intersex] is quite common in infancy and adolescence.
While it is obvious that an infant cannot give informed consent, intersex surgeries in adolescence also follow highly coercive patterns, quite apart from general questions as to an appropriate age for consent for various kinds of medical procedures. Far from involving informed consent, for example, gonadectomies commonly done on female-assigned intersex youth were based on total deception. For example, girls with Complete Androgen Insufficiency were told that they had “ovarian cancer,” and were going to have their ovaries removed: better to raise the nonexistent specter of a life-threatening disease than to permit a young adult to learn that she is intersex. The deception was for her “protection”. Likewise, vaginoplasty is often presented as a given to a young woman, who may be invited to give some input as to the type of procedure, as opposed to whether she desires surgery in the first place. Fully informed consent, including support for the young person’s express right to reject surgery even if the parents are enthusiastically in favor, is the rare exception rather than the rule.
As an organization committed to informed consent as a prerequisite to ethical sex [re]assignment surgery, WPATH must therefore join the intersex community, and human rights forums including the UN and EU, in opposing IGM and calling for all nations to follow the example of Malta and Chile in outlawing this violent form of child abuse.
As an organization dedicated to the well-being and human dignity of sex and gender variant people, WPATH should above all oppose IGM for the same reasons as FGM. It at once reflects social stigma and reinforces it with the physical pain and lifelong psychological trauma of genital cutting, while risking and often, in fact, impairing sexual sensitivity. It is indeed a form of childhood sexual abuse that keeps on violating the survivor’s bodily and sexual self-determination in adulthood, regardless of the intersex person’s gender identity or sexual orientation. Indeed, the professional superstition and hubris behind IGM may be comparable to that behind clitoridectomies performed in the UK and USA during the 19th century to cure “certain forms of hysteria, insanity, and epilepsy in women.” [1]. Just as the medical profession ultimately rejected this form of “therapeutic” FGM, so the similar violence of IGM must be decisively rejected. with WPATH in a vitally important leadership position.
Additionally, IGM may cause extra dysphoria and complications for the survivor who turns out not to identify with their assigned sex, rather as FGM may create special complications for the survivor who turns out to identify as a trans man. An organization concerned with the treatment of gender dysphoria may well take note of these special iatrogenic harms. However, neither FGM nor IGM is primarily an issue of “gender identity,” but of the purposeless infliction of stigma, suffering, and impairment of sexual feeling (whether as the main purpose or predictable “collateral damage”) without the patient’s informed consent. Only an intersex person’s autonomous desire and fully informed consent at an appropriate age can justify such genital surgeries.
It is imperative that WPATH be as forthright and assertive in affirming these simple ethical standards as it is, for example, in opposing immediate surgery for endosex children who may express a strong desire to transition in every way, with enthusiastic support from their parents. The message, otherwise, is that intersex people are of a lesser kind, whose personal and bodily autonomy does not really count. The adage that “silence is consent” is all too appropriate where intersex medical child abuse is concerned.
At Boston in 1996, medical professionals chose to circulate press releases stating how much they cared about their pediatric intersex patients while refusing to meet with former patients who had experienced IGM and fairly listen to their side of the story. Two decades later, WPATH can and must do better by meeting with the intersex community it has injured and collaborating with them on a plan to remedy the damage done and advance the global struggle by OII and other intersex activists to outlaw IGM throughout the globe.
Removing “Disorders of Sex Development” from the Standards of Care: Depathologizing intersex
Language counts, and good intentions will not avoid the harm done to intersex people and communities by the misbegotten phrase “Disorders of Sex Development” (DSD). While noting that “[s]ome people object strongly to the ‘disorder’ label, preferring instead to view these congenital conditions as a matter of diversity… and to continue using the terms _intersex_ or _intersexuality_” (with the former now generally preferred by intersex people and allies), WPATH attempts to justify its DSD usage:
“WPATH uses the term DSD in an objective and value-free manner, with the goal of ensuring that health professionals recognize this medical term and use it to access relevant literature as the field progresses. WPATH remains open to new terminology that will further illuminate the experience of members of this diverse population and lead to improvements in health care access and delivery.” – Standards of Care, Section XV, p. 207
As the intersex community and organizations such as OII have been declaring for many years, the way for WPATH to adopt “new terminology that will further illuminate the experience of members of this diverse population” is to go back to the future: intersex is the appropriate term! Endosex trans allies must insist on this, with the pro-IGM poster session at Amsterdam as an object lesson of where DSD language and concepts all too easily lead us.
Closely following the above quotation on the allegedly “objective and value-free” use of DSD language, WPATH notes the proposal currently in 2011 for DSM-5, and since adopted, “to replace the term gender identity disorder with gender dysphoria.” (Ibid. at 208.) So it would seem that the term “disorder” is not so objective or value-free when applied to trans people, whether endosex or intersex. If the term is objectionable when applied to gender variant people, and thus worth changing, it is at least equally objectionable when applied to intersex people generally.
Using the simple and highly recognizable term intersex, and noting where necessary that the historical literature includes terms such as “gender identity disorder” (GID) and “disorders of sex development” (DSD) now rightly replaced with non-pathologizing and inclusive language to recognize these human variations, is an approach allowing readers “to access relevant literature” while also promoting human dignity and understanding for intersex and/or trans people. And human dignity and understanding are critically important ingredients in seeking “improvements in health care access and delivery.”
Why WPATH has chosen to use DSD language is an open question. Either sheer inertia and deference to prevailing jargon, or a more considered decision to “go along in order to get along” with certain colleagues, are possibilities. The latter tendency may explain, for example, the defense by professionals who should know better of colleagues who have imposed reparative and often highly coercive “therapies” on trans and gender nonconforming children — despite that clear and commendable message of WPATH that such methods are futile, harmful, and also highly unethical. In the case of intersex children, we are confronted with “conversion therapists” like those presenting the poster session on “DSD” in Amsterdam, who are armed with scalpels.
While it is easy for allies to inform WPATH that intersex is the correct and responsible term to use, and terms such as intersex variations for the range of sex characteristics and patterns of variation that intersex people may manifest, as opposed to the language of “disorders,” only the intersex community itself can negotiate with WPATH a process of improving the Standards of Care which takes into account the experience of intersex people, trans or otherwise. We join the intersex community in demanding that such a dialogue promptly take place, leading to a new version of Section XV and possibly other relevant portions of the Standards of Care released at the earliest possible date to address past injuries including the recent poster session, and to move in a constructive direction in the timely way that the urgency of the situation requires.
Intersex people who transition: Affirmative action by WPATH
The simple actions of condemning IGM and its contribution to the iatrogenic manufacture and aggravation of sex dysphoria, and replacing harmful DSD terminology with intersex-friendly language (including the word intersex itself!), will do much to bring WPATH into compliance with the precept of the Hippocratic Oath: “First, do no harm.”
However, WPATH’s obligations in its role of professional leadership go far beyond that: it has taken on the responsibility to see that all trans people, including intersex trans people, receive medically informed and culturally appropriate care. This means especially that professionals who deal with trans people and transition care must be informed both as to the nature of intersex variations of different kinds, and the experiences of intersex people (whether IGM survivors or otherwise) who consider or seek out medical and social gender transitions of different kinds.
Given WPATH’s increased responsiveness to the realities and needs of nonbinary trans people in Version 7 of the Standards of Care, it is only appropriate that a dialogue with the intersex community include full recognition of nonbinary intersex people such as Viloria and Zzyym, among whom some seek medical transition as well as social and/or legal recognition of their nonbinary identities. Likewise, some but not all endosex trans people with non-binary identities seek medical transition through hormones and/or surgery.
In this pursuit of inclusiveness and excellence, only active dialogue with intersex trans people, and a thorough rewriting and expansion of Section XV to reflect this vast range of first-hand experience will do. The revolutionary insights and improvements growing out of such a process of dialogue and incorporated of lived experience may be comparable to changes in women’s, LGBTIQA, and trans health care models and delivery brought about by feminist, LGBTIQA, and trans activism and advocacy over the last half-century.
Outrage at the Amsterdam poster session promoting IGM is the catalyst bringing home the need for this revolution, which yet is also promised on the abiding hope that WPATH will act in accord with its best human values as well as its highest standards of professional excellence in joining the international struggle against FGM and IGM alike, and indeed fostering “improvements in health care access and delivery” for all trans and gender nonconforming people, including those who are intersex and face unique additional challenges and oppressions where all trans people and WPATH professionals should be informed and committed allies.
Acknowledgment: Warmest thanks to Cary Gabriel Costello of The Intersex Roadshow and TransFusion for their invaluable feedback and suggestions, many of which are incorporated in my article, with the caution that any flaws or infelicities are solely my responsibility.
Margo Schulter is a pioneering trans Lesbian feminist and moderator of the Conversations Project‘s community group.
Koomah is an intersex educator, co-founder of Houston’s intersex group, moderator of the Conversations Project community group, and board member of TFA, the TransAdvocate’s parent organization.
- See, e.g., Ruth Herschberger, _Adam’s Rib_ (1948; reprinted by Harper and Row, New York, 1970), pp. 126-129 and p. 222, nn. 3-7



Of course the majority of intersex people identify as the gender they were born as and thus experience Cis privilege. Many of them have difficulty admitting that and it’s a reason why I struggle to be an ally.
We even managed to produce a guidance calling WPATH to apply strict bioethical criteria for posters and presentations in future conferences, it was presented at the final plenary, and it will be implemented in the upcoming EPATH Conference.
Trans and Intersex activists worked together at WPATH in Amsterdam, in regard to the poster that you mention, but also in regard to other presentations -including the session on DSD at 8 am in the morning, attending for many trans activists supporting intersex colleagues, and we worked together preparing visual manifestos for that session. Actually, most intersex activists attending WPATH in Amsterdam were invited by GATE (a trans international organization), including intersex activists from the US, Australia, The Netherlands, South Africa, China and México, but none of them is quoted in your article about what happened there. I don’t fully understand why you talk about a ” crisis of confidence and trust between the intersex and trans communities”, because the WPATH conference showed a strong alliance between them.